
{kind=link}

Super User
Full dose Sofosbuvir is safe and effective in patients with renal failure +/- dialysis

When sofosbuvir first reached the market it was not approved for patients with CKD (Chronic Kidney Disease) stages 4 and 5 which means patients with an eGFR of < 30 ml/min. This was based on the observations that:
- Sofosbuvir is rapidly metabolised to GS-331007 (t1/2 0.4 hours), and
- GS-331007 (t1/2 27 hours) has renal excretion, and
- In the context of a reduced eGFR the AUC (Area Under The Curve) for this metabolite rises substantially
The concern was that the higher levels of GS-331007 might be toxic. This presents a real problem in countries that are dependent on generic DAA medication for HCV treatment because all these regimens are based on Sofosbuvir. There are currently no generic versions of Mavyret or Zepatier.
The short story is that experimentation has shown the following:
- The higher levels of the GS-331007 in patients with CKD are not toxic
- GS-331007 is cleared by haemodialysis or by the remaining GFR
- Reduced dose sofosbuvir (ie 200 mg daily) results in poor SVR12 rates (<50%) in patients with CKD
- Full dose sofosbuvir (ie 400mg daily) results in normal SVR12 rates (~95%) in patients with CKD +/- dialysis without problematic side effects
Here is a non-exhaustive list of published studies showing the use of full-dose sofosbuvir in patients with CKD is safe and effective:
- AASLD 2018 - Sofosbuvir/Velpatasvir for 12 Weeks Is Safe and Effective in Patients Undergoing Dialysis
- Hepatology Communications 2017 - Sofosbuvir‐based regimens for the treatment of chronic hepatitis C in severe renal dysfunction
- J Clin Transl Hepatol. - Sofosbuvir Use in the Setting of End-stage Renal Disease: A Single Center Experience
- Kidney Int Rep. - Hemodialysis Patients Treated for Hepatitis C Using a Sofosbuvir-based Regimen
- Indian J Gastroenterol. - Efficacy and safety of sofosbuvir-based regimens in chronic hepatitis C patients on dialysis
- Liver Int. - Sofosbuvir-based treatment is safe and effective in patients with chronic hepatitis C infection and end-stage renal disease: a case series
- J Hepatol. - Pharmacokinetics, safety and efficacy of a full dose sofosbuvir-based regimen given daily in hemodialysis patients with chronic hepatitis C
So, although the current EASL and AASLD guidelines suggest using an alternative to Sofosbuvir, these guidelines were written by people in live in countries with the luxury of having alternatives.
Where alternatives to Sofosbuvir are not available there is sufficient evidence in the public domain indicating it is safe to use Sofosbuvir in CKD, which, to me, makes it ethical given the usual benefits exceed the risks equation we all use to guide our clinical practice.
For those who are interested why here is the explanation.
Sofosbuvir is not an active drug. It is a prodrug that requires activation. This activation happens as follows:
- The concentration gradient of the Sofosbuvir prodrug depends almost entirely on the Cmax (rather than the AUC) so, in line with usual pharmacokinetics, the higher the dose administered the higher the Cmax
- The higher the concentration, the more Sofosbuvir penetrates the target cells as there is a higher concentration gradient driving this influx
- Once the sofosbuvir is intracellular it is cleaved and phosphorylated into the active entity which is a polar charged molecule trapped in the cell
In other words, Sofosbuvir is like Gentamicin where it is the Cmax peak that determines efficacy, not the AUC.
Reducing the administered Sofosbuvir dose
- reduces the Cmax, which
- reduces the concentration gradient driving it into target cells, which
- reduces the intracellular levels of the active cleaved/phosphorylated form and in turn
- reduces the time that this level exceeds the EC50
This also explains the lower efficacy in cirrhotic patients. Fibrous scar tissue has a reduced blood supply, this reduces the effective concentration gradient driving the Sofosbuvir into cells due to a dynamic depletion effect - although the concentration in the blood is the same, the small quantity of blood soon runs out of Sofosbuvir...
So while for many renally cleared drugs (including Ribavirin) we do need to decrease the dose in CKD we do not want to do this with Sofosbuvir. Fortunately for patients, the circulating metabolite that is renally cleared (GS-331007) has been proven to be non-toxic so the fact it will be circulating at higher levels in patients with CKD can be safely ignored. This metabolite is cleared by either a low eGFR or dialysis.
Unfortunately, I can't share it here at the moment, because it is in publication as we speak, but I am aware of a large multicentre trial in patients with CKD and haemodialysis who were given full dose Sofosbuvir 400 mg / Daclatasvir 60 mg daily and achieved 98% SVR12.
Sound Therapy for Tinnitus

Perhaps it's age, perhaps it's Hep C, perhaps it's the medication. Whatever the reason, the reality is quite a few people with Hep C have issues with tinnitus. A friend of mine called Davo had this issue and resorted to Google where he found an Australian company called "Sound Therapy International". Lucky it was him, rather than me, as I tend to think anyone who calls them self International is about as "International" as the Democratic People's Republic of Korea is "Democratic". Anyway, I digress.
As a doctor I know we don't have a lot to offer drugs or surgery wise to help patients with tinnitus, so when he told me that it's
- Not that expensive (not sure I agree on that one)
- Has reduced his tinnitus to such an extent it's pretty much gone
- Has had other benefits around sleep and general well being
He had my attention because Davo is rather inclined to call it as he sees it, and not prone to sugar coating stuff.
So, it's a case study of 1, and your results may differ.
It's also not cheap in that the basic package is $699 AUD ($500 USD) which seems quite a lot to pay for a few books, some headphones and what is essentially an MP3 player.
That said the results are currently 100% (1/1) (95% Confidence Interval 2.5-100%) so if you suffer from this debilitating problem maybe it's worth a try?
It's not one of the affiliate things where we ask you to tell them we sent you so we can collect a commission, but if you do decide to give it a try I'd be really interested to hear your results. It would be interesting to know how well this actually works and it seems reasonably common with HCV.
Maviret (Mavyret) is an awesome drug for HCV
It's come to my attention that some people on the Internet are "bad-mouthing" Maviret (Mavyret) and suggesting it's the worst option on the market and that you need Sofosbuvir. Anyone stating this does not, as they say, know their ass from their elbow - this drug is awesome where awesome means great cure rates, short duration of treatment, and minimal side effects. While there is no doubt Sofosbuvir based regimens are also great there are very few patients for whom they might be superior.
Let's start with the spelling. Is it Maviret or Mavyret? The answer is it's both! The combination of Pibrentasvir and Glecaprevir from Abbive goes by both names, depending on the market. Let's call it G/P for short, after all, that's what most doctors call it.
Common things happen commonly
Now let's have a look at the profile that fits the vast majority of patients - treatment naive, low fibrosis. Here is a link to the seminal study in the Journal of Hepatology: https://www.journal-of-hepatology.eu/article/S0168-8278(18)30165-X/fulltext looking at the results for G/P

And I could probably stop here because let's face it, that's pretty amazing. Did I mention this G/P combination is awesome?
Now, by way of comparison let's pull out Gilead's latest and greatest 2 drug combination - Epclusa - aka Sofosbuvir + Velpatasvir. How does that perform in the most common case?
Here it is: http://www.natap.org/2016/DDW/DDW_13.htm and looking at the SVR12 results we see:
Hmm, that looks similar but, dare I say, a little worse. Not quite as good in the most common GT1 patients, or the next most common GT3 patients, or the next most common GT2 patients. Now don't get me wrong, it's far from shabby and there is, in fact, no statistical difference but it does rather put to rest the notion that G/P is inferior.
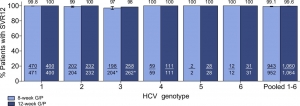
Patients with cirrhosis
Ok, so let's dig into the hard cases -patients with cirrhosis. For G/P in GT1,2,4,5,6 it looks like this http://www.natap.org/2018/AASLD/AASLD_17.htm
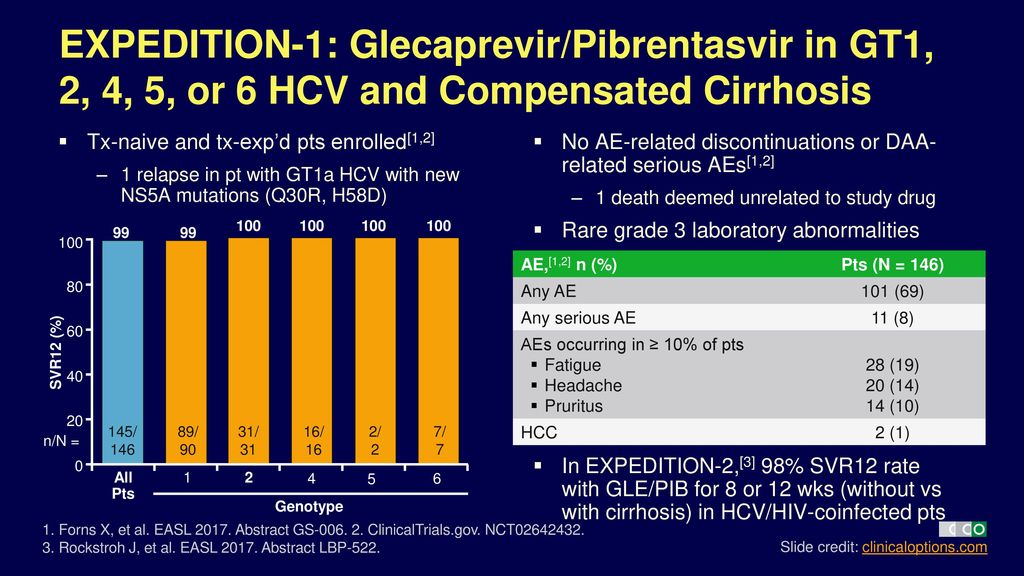
There's not a lot to say about that other than it's not what we usually expect with significantly reduced SVR12 in patients with cirrhosis.
GT3 Cirrhotic Patients
And, finally, let's get into the really hard basket - GT3 patients with cirrhosis +/- treatment experience
For G/P in GT3 with cirrhosis +/- treatment experience it looks like this: http://www.natap.org/2017/HCV/092217_01.htm
Does a sofosbuvir based regimen have any advantages over G/P?
So do Sofosbuvir based regimens have any advantages over G/P? Yes, there are several special use cases for it. For example, G/P can't be given to people with decompensated cirrhosis, whereas Sofosbuvir-based regimens can: http://www.natap.org/2015/AASLD/AASLD_64.htm and they work pretty well:
There are a few other circumstances where you would prefer a sofosbuvir-based regimen but these are rare and relate to treatment experience and retreatment and in this case you should be consulting an expert for advice, not the Internet.
Conclusions
Personally, I'd be happy to have either G/P or a Sofosbuvir based regimen. I would not be at all worried about being prescribed G/P, in fact I might well secretly be pleased, not only because of the short duration and favourable side effect profile but because if you add Sofosbuvir to G/P you have the most potent 3 drug combination for HCV that is available, ideal for retreatment, but that, as they say, is a story for another day.
83 Hepatitis C Studies From AASLD 2018

For the past 2 decades, Jules Levin at NATAP has done a fantastic job reporting what is presented at all the major scientific meetings on HIV, HBV and HCV around the world.
Here are 83 studies presented at the AASLD 2018 conference that cover the leading edge of Hep C research as it currently stands.
- Hepatitis Debrief: The Liver Meeting 2018 - (11/19/18)
- DAA HCV Retreatment Studies at AASLD 2018 - (12/07/18)
- Changing Cascade of Care for Hepatitis C in the Era of Direct-Acting Antivirals - (11/13/18)
- Impact of all-oral direct-acting antivirals on clinical and economic outcomes in chronic hepatitis C virus-infected patients in the U.S. - (11/13/18)
- Disparities in Accessing HCV Care under Medicaid Programs Across the US; Experience from the TRIO Network - (12/10/18)
- Universal HCV Screening on the Way? - (11/13/18)
- Hepatitis C Risk-Based vs. Universal Screening Among Pregnant Women: Implementation and Cost-Effectiveness Analysis - (11/19/18)
- Prevalence of Chronic Hepatitis C Virus Infection US States and District of Columbia, 2013-2016 - (12/10/18)
- A REAL WORLD RESISTANCE PROFILE OF VIROLOGIC FAILURES COLLECTED FROM AN INTERNATIONAL COLLABORATION (SHARED) - (12/10/18)
- Prevalence of NS3 and NS5A resistance-associated substitutions through European DAA-failures - (12/10/18)
- The prevalence of hepatitis C virus NS5A polymorphisms in Europe - (12/10/18)
- Endothelial function worsens with hepatitis C direct-acting antiviral treatment despite improvements in systemic measures of inflammation - (11/28/18)
- Baseline Polymorphisms and Phylogeographic Analysis of NS3, NS5A, and NS5B in HCV Genotype 1b-Infected Chinese Patients Enrolled in ONYX-1 - (11/28/18)
- Clinical Benefits, Economic Savings and Faster Time to HCV Elimination with a Simplified 8-Week Treatment and Monitoring Program in Chronic F0-F3 Naïve Patients in the US - (11/28/18)
- Effectiveness and Safety of DAA Treatment for CHC Patients with Previous HCC: A REAL-C Study - (11/28/18)
- Drug-Drug Interaction Potential of Glecaprevir/Pibrentasvir Based on Real-World Medication Use in Patients With Chronic Hepatitis C Virus Infection: Data From the German Hepatitis C-Registry (DHC-R) and PAN-Cohort - (11/27/18)
- Effectiveness of Sofosbuvir / Velpatasvir in Treating Hepatitis C Virus Infection in Real-world Setting / IDUs, British Columbia - (11/27/18)
- GLECAPREVIR/PIBRENTASVIR ADMINISTERED FOR 8 WEEKS RESULTS IN EXCELLENT EFFECTIVENESS AND SAFETY: A REAL-LIFE STUDY ON 639 ITALIAN HCV PATIENTS FROM THE NAVIGATOR LOMBARDIA NETWORK - (11/26/18)
- Treatment of Genotype 3 Cirrhotic patients with 12 weeks Sofosbuvir/Velpatasvir with or without ribavirin: Real life experience from Italy - (11/26/18)
- Improved Short-Term Survival in HCV Seropositive Kidney Transplant Recipients during the DAA Era in the United States - (11/26/18)
- Uptake of and factors associated with direct-acting antiviral therapy among patients in the CHeCS, 2014-2017 - (11/26/18)
- Risk-Based HCC Surveillance Strategies Using HCC Risk Prediction Models Have Greater Net Benefit Than the Current One-Size-Fits-All Strategy In Patients who Received Antiviral Treatment for HCV - (11/26/18)
- Preemptive DAA Therapy in Donor HCV-positive to Recipient HCV-negative Cardiac Transplantation - (11/19/18)
- HCV-RNA Is Readily Detectable in Nasal and Rectal Fluids of HCV Patients with High Viremia - (11/19/18)
- High SVR in PWID with HCV Despite Imperfect Medication Adherence: Data from the ANCHOR Study - (11/20/18)
- The Hepatitis C Continuum of Care for People Who Inject Drugs; Philadelphia, PA - young PWID 8% treated for HCV, older still only 25% - (11/20/18)
- Risk of Incident Diabetes in Hepatitis C Patients Following Completion of Direct-acting Antiviral Therapy - (11/19/18)
- The impact of HCV SVR from direct acting antiviral and interferon-based treatments on mortality in a large population based cohort study - (11/19/18)
- Hepatitis C Risk-Based vs. Universal Screening Among Pregnant Women: Implementation and Cost-Effectiveness Analysis - (11/19/18)
- Direct Antiviral Agents after Successfully Treated Early Hepatocellular Carcinoma Improve Survival in Cirrhotic Patients with Chronic Hepatitis C - (11/19/18)
- Sustained Virologic Response Reduces the Incidence of Extrahepatic Manifestations in Chronic Hepatitis C Infection - (11/16/18)
- Impact of Baseline HCV RNA Levels as Assessed by 2 Different Assays on the Efficacy of 8-Week Glecaprevir/Pibrentasvir in Patients With HCV GT1-6 Infection - (11/16/18)
- Risk of Cardiovascular Disease Events after HCV Treatment: Results from ERCHIVES - (11/16/18)
- Effectiveness of 8-week glecaprevir/pibrentasvir(G/P) for treatment naïve, non-cirrhotic patients with HCV infection in the TRIO Health network - (11/16/18)
- Sofosbuvir/Velpatasvir/Voxilaprevir (SOF/VEL/VOX) for Prior Treatment Failures with Glecaprevir/Pibrentasvir (G/P) in Chronic Hepatitis C Infection - (11/16/18)
- REAL-WORLD SAFETY AND EFFECTIVENESS OF SOFOSBUVIR/VELPATASVIR/VOXILAPREVIR AND GLECAPREVIR/PIBRENTASVIR IN HEPATITIS C INFECTED PATIENTS - (11/16/18)
- HEPATITIS C VIRUS REINFECTION AND INJECTING RISK BEHAVIOR FOLLOWING ELBASVIR/GRAZOPREVIR TREATMENT IN PARTICIPANTS ON OPIATE AGONIST THERAPY: C-EDGE CO-STAR PART B - (11/16/18)
- Pharmacokinetics of Once-Daily Sofosbuvir or Ledipasvir/Sofosbuvir in HCV-Infected Pediatrics Aged 3-<6 Years - (11/16/18)
- Ledipasvir/Sofosbuvir for 12 Weeks Is Safe and Effective in Children 3 to <6 years old with Chronic Hepatitis C Virus Infection - (11/16/18)
- Efficacy and Safety of Glecaprevir/Pibrentasvir in Patients With Chronic HCV Infection and Moderate to Severe Renal Impairment: An Integrated Analysis - (11/16/18)
- Durability of Sustained Virologic Response and Liver-Related Safety in Patients Treated With Glecaprevir/Pibrentasvir: A Long-Term Follow-Up Study - (11/16/18)
- Sofosbuvir / Velpatasvir / Voxilaprevir in DAA Failure Patients with Cirrhosis. Final Results of the French Compassionate Use Program - (11/16/18)
- Retreatment with voxilaprevir/velpatasvir/sofosbuvir in patients with chronic hepatitis C virus infection and prior DAA failure - results from the German Hepatitis C-Registry (DHC-R) - (11/16/18)
- Safety and Efficacy of Sofosbuvir/Velpatasvir in Genotype 1-6 HCV-Infected Patients in China: Results From a Phase 3 Clinical Trial - (11/16/18)
- High SVR in PWID with HCV Despite Imperfect Medication Adherence: Data from the ANCHOR Study updated - (11/16/18)
- Safety and Efficacy of Sofosbuvir/Velpatasvir in Genotype 1-6 HCV-Infected Patients in China: Results From a Phase 3 Clinical Trial - (11/19/18)
- Incidence and Predictors of de Novo Hepatocellular Carcinoma Following Achievement of Sustained Virologic Response With Direct-Acting Antivirals: Results From the Gilead SVR and Cirrhosis Registries - (11/14/18)
- Retreatment with SOF/VEL/VOX in Treatment-Experienced Patients with and without HIV: The RESOLVE Study - (11/14/18)
- Effectiveness of Elbasvir/Grazoprevir in Black Persons With Genotype 1 Hepatitis C Virus - (11/14/18)
- Efficacy and Safety of Elbasvir/Grazoprevir for 8 or 12 Weeks in Participants With Hepatitis C Virus Genotype 4 Infection - (11/14/18)
- Utilization and Effectiveness of Elbasvir/Grazoprevir for the Treatment of Hepatitis C Virus Genotype 1b Infection: Updated Cohort From the US Veteran Affairs Healthcare System - (11/14/18)
- Sofosbuvir/Velpatasvir for Patients With Chronic Genotype 3 HCV Infection With Compensated Cirrhosis: an Integrated Analysis of Phase 2 and Phase 3 Clinical Trials - (11/14/18)
- Effectiveness of Sofosbuvir/Velpatasvir for 12 Weeks in HCV Genotype 3 Patients with Compensated Cirrhosis in Clinical Practice Cohorts from Around the World - (11/14/18)
- Sustained Viral Response Following Treatment With Direct-Acting Antiviral Regimens Is Durable in More Than 6600 Patients: Results of the Gilead Sustained Virologic Response Registry Study - (11/14/18)
- Efficacy and Safety of 8 Weeks of Glecaprevir/Pibrentasvir in Treatment-Naïve Adults With HCV Genotype 1-6 and Aspartate Aminotransferase to Platelet Ratio Index (APRI) ≤1 - (11/14/18)
- Response-Guided Therapy with DAA Shortens Treatment Duration in 50% of HCV Treated Patients - (11/14/18)
- Early Treatment with Direct-Acting Antivirals Saves Medical Costs in Non-Cirrhotic Patients with Chronic Hepatitis C Virus Infection in the United States - (11/14/18)
- Nivolumab in Patients With Child-Pugh B Advanced Hepatocellular Carcinoma in the CheckMate040 Study - (11/13/18)
- Changes in the characteristics of hepatitis C patients treated with direct-acting antivirals from 2014-2017 - (11/13/18)
- Short-Duration Sofosbuvir/Velpatasvir Safe and Effective in Treating HCV Infection Immediately After Liver Transplant - (11/13/18)
- Efficacy and Safety of Glecaprevir/Pibrentasvir in Patients With HCV Genotype 5 or 6 Infection: Final Results of the ENDURANCE-5,6 Study - (11/13/18)
- Changing Cascade of Care for Hepatitis C in the Era of Direct-Acting Antivirals - (11/13/18)
- Quality of Life in Patients with Psychiatric Disorders: Pooled Analysis from Glecaprevir/Pibrentasvir Registrational Studies - (11/13/18)
- Real-World Effectiveness of Glecaprevir/Pibrentasvir in 1,941 Patients with Hepatitis C Genotypes 1 through 4 - (11/13/18)
- Lower Likelihood of Graft Failure and Death after Liver Transplantation in the Era of Current Direct Acting Antivirals: An Analysis of the 2002-2018 United Network for Organ Sharing Registry - (11/13/18)
- Impact of all-oral direct-acting antivirals on clinical and economic outcomes in chronic hepatitis C virus-infected patients in the U.S. - (11/13/18)
- High efficacy of glecaprevir/pibrentasvir in patients with chronic HCV GT1 infection who failed prior treatment with NS5A-inhibitor plus sofosbuvir regimens - (11/13/18)
- Sofosbuvir/Velpatasvir for 12 Weeks Is Safe and Effective in Patients Undergoing Dialysis - (11/13/18)
- The impact of HCV SVR from direct acting antiviral and interferon-based treatments on mortality in a large population based cohort study - (11/13/18)
- PRELIMINARY EFFICACY AND SAFETY OF 8-WEEK GLECAPREVIR/PIBRENTASVIR IN PATIENTS WITH HCV GENOTYPE 1-6 INFECTION AND COMPENSATED CIRRHOSIS: THE EXPEDITION-8 STUDY - (11/13/18)
- Real World Effectiveness of Sofosbuvir/velpatasvir/voxilaprevir in 573 Treatment-Experienced Patients with Hepatitis C - (11/13/18)
- High SVR in PWID with HCV Despite Imperfect Medication Adherence: Data from the ANCHOR Study - (11/13/18)
- Retreatment with SOF/VEL/VOX in Treatment-Experienced Patients with and without HIV: The RESOLVE Study - (11/13/18)
- Incidence of Hepatocellular Carcinoma Among Patients With Hepatitis C Virus Infection Following Treatment With a Grazoprevir-Containing Regimen - (11/13/18)
- Real-World Impact of Resistance-Associated Substitutions on Re-Treatment after Ledipasvir/Sofosbuvir Virologic Failure in Hepatitis C Patients (VA) - (11/13/18)
- The Medicines Patent Pool Signs Licence with AbbVie to Expand Access to Key Hepatitis C Treatment, Glecaprevir/Pibrentasvir - (11/13/18)
- Universal HCV Screening on the Way? - (11/13/18)
- Real-life effectiveness and safety of velpatasvir/sofosbuvir/voxilaprevir for previously DAA treated patients with chronic hepatitis C - (11/13/18)
- Sofosbuvir/velpatasvir/voxilaprevir(SOF/VEL/VOX) in care of chronic hepatitis C patients; clinical practice experience from the TRIO network - (11/13/18)
- Glecaprevir/Pibrentasvir for the Treatment of Patients With Chronic Hepatitis C Virus Infection: Updated Real-World Data From the German Hepatitis C-Registry - (11/11/18)
- National Estimates for HCV Screening and Diagnosis Rates in the United States (2013-2016) Based on a Large Real-World Dataset - (11/11/18)
- National Examination of HCV Linkage to Care in the United States (2013-2016) Based on Large Real-World Dataset - (11/09/18)
- AbbVie Characterizes Evolving Hepatitis C (HCV) Patient Landscape in the United States Using Comprehensive Dataset - (11/09/18)
PHARMAC announces funded Maviret from Feb 1st 2019

In an announcement worthy of 3 dancing bananas  , PHARMAC in New Zealand have just announced:
, PHARMAC in New Zealand have just announced:
We are pleased to announce a decision to fund a new treatment for chronic hepatitis C infection, glecaprevir and pibrentasvir (Maviret) from 1 February 2019, and to widen access to adalimumab (Humira) for patients with psoriasis from 1 July 2019, through an agreement with AbbVie Ltd.
In summary, this decision will result in the following:
On 1 February 2019:
- Glecaprevir with pibrentasvir (Maviret) tablets will be funded in the community and DHB hospitals without restrictions for patients with chronic hepatitis C. Maviret treats all genotypes of hepatitis C.
- Maviret will replace the currently funded open-listed hepatitis C treatment, Viekira Pak (+/- RBV), which will be delisted on the same day. Viekira Pak can only be used to treat patients with genotype 1 hepatitis C.
For more details see the attached press release.
Clinical Impact of New Viral Hepatitis Data From AASLD 2018
Here is a summary slide set where expert faculty members summarize key viral hepatitis studies from AASLD 2018 in San Francisco. Use these slides to review data on newer HCV regimens, the HCV continuum of care, posttreatment HCV outcomes, HCV D+R- transplantation, NA cessation in chronic hepatitis B, and investigational HBV/HDV therapeutics.
Understanding Viral Load and Hepatitis C Treatment Success
The usual way we detect Hepatitis C is using an Antibody test. Following infection with Hepatitis C the body forms antibodies to the virus and these antibodies persist lifelong. In about 25% of patients the antibodies successfully remove the virus, however, the remaining 75% of patients go on to develop chronic Hepatitis C (persistent infection).
Counting how many of the Hepatitis C virus particles are present in a patient's blood is possible through the Quantitative HCV PCR RNA test, the result is called Viral Load, and is usually measured in IU/mL (international units per millilitre) although some laboratories use copies/ml. Most patients believe that a low viral load pre-treatment (less than 800,000 IU/L) is good since a smaller virus count should, in theory, translate to less liver damage, and should make it easier to achieve cure, while many with high viral loads are worried that their treatment may not work. But is any of this actually true? With the advent of the newer HCV medications, the answer is no, none of it is. Strange as it may seem, your viral load has very little correlation to either liver damage or cure rate. Patients with very high viral loads have the same excellent cure chances as anyone else, 95% for Genotypes 1,2,4,5,6 and 90% for Genotype 3, when treated with the modern direct-acting antiviral medications, or DAAs (e.g. Harvoni®, Epclusa®, Mavyret®, Zepatier®).
A high viral load pre-treatment may not be a bad thing
You have a high viral load because your body (immune system) is not really trying to do much. The upside is that less liver damage occurs because your immune system is not destroying your liver in its attempt to kill the virus. The downside is that, well, actually there is no downside, besides the extra ink to print the extra zero after the average 1-3 million viral load. 10 million viruses, for example, don't eat much, maybe half a hamburger a year, they are very small, so you can afford to feed them.
Additionally, both low and high viral load patients respond extremely well to the new DAAs. It's common to see a patient with a 10 million viral load fall below 1000 in the first week of treatment - these drugs are remarkably effective.
Viral load monitoring after start of treatment
DAA medications do not require a lot of monitoring (unless Ribavirin® is involved). After starting treatment, viral loads decline quickly and profoundly. The data indicates that almost 100% of patients taking DAA drugs will suppress the virus to incredibly low levels and generally do this very quickly. At week 4 of the standard 12 weeks treatment, a whopping 82% of patients will become undetectable (UND). Once you fall to UND, you will remain UND for the duration of treatment, so further measurements are a waste of time and money.
Eventually, we may only do one HCV viral load test after commencing treatment, either 12 or 24 weeks post-treatment. For now it is very reasonable to do the test at week 4 (mostly for your peace of mind) and then 12 or 24 weeks post-treatment.
It's worth noting that patients should not be too alarmed if their viral load remains detectable at week 4, or even at end of treatment, as there is still a high likelihood of being cured. When treated with DAAs, having low-level detectable HCV RNA at the end of treatment does not preclude cure and several studies have duplicated this result. Some specialists advise patients who are still detected at week 4 to extend their treatment to 16-24 weeks (instead of 12) as extra insurance, while others see no benefit in doing this, so there is no consensus on this point. However, if money is no object, or if you can access high-quality generics, extending treatment is known to add a small single digit % to cure rates.
When can a patient be declared cured?
At the end of treatment, one of two things will happen. If there is any remaining viable virus then it will begin growing back. This will start as soon as the treatment medications wash out of a patients system (about 1 week to fall below any useful level).
Patients should take either a Qualitative HCV PCR RNA test or a Quantitative HCV PCR RNA 12 weeks after the end of treatment to learn if they were cured. Cure can be declared with 99.7% certainty when a patient has an undetectable test 12 weeks after end of treatment (SVR12 - Sustained Virological Response @ 12 weeks). The certainty increases to 99.99% when the test yields an undetectable result 24 weeks after end of treatment (SVR 24) and is the gold standard for declaring a patient cured.
It's worth noting that patients will continue to have a positive HCV antibody test. This is the marker of exposure to the disease, not of current infection.
Waiting 12 or 24 weeks after end of treatment to learn the outcome can be understandably nerve-racking, even with cure rates as high as 95%+ with the new DAA medicines. So the results of this large trial may provide some relief. Investigators have calculated the consistency between SVR at 4 weeks post-treatment (SVR4) and SVR at 12 weeks post-treatment (SVR12), as well as between SVR12 and SVR24. Overall, 98.0% of patients with an SVR4 also achieved an SVR12, and 99.7% of patients with an SVR12 also achieved an SVR24. As a side note, of patients who relapsed post-treatment, 77.6% did so within 4 weeks of finishing treatment.
Conclusions
Contrary to common belief, a viral load result does not predict a patient's cure chances, nor does it provide any information about the condition of his/her liver or level of scarring. It's a number that is used to monitor a patient's progress during treatment by measuring it at baseline (before starting treatment), then again during treatment to learn how patients are responding to the medications. When treated with the modern Hep C medications, patients with very high viral loads have the same extremely high cure chances of those with low viral loads. Only the HCV PCR RNA test can be used to assess cure as the Antibody test used for screening is expected to remain positive.
Generic Mavyret (Maviret) Coming Soon!
The Medicines Patent Pool Signs Licence with AbbVie to Expand Access to Key Hepatitis C Treatment, Glecaprevir/Pibrentasvir
SAN FRANCISCO, November 12, 2018 /PRNewswire/ --
Important collaboration will ensure affordable hepatitis C treatment options in low- and middle-income countries.
The Medicines Patent Pool (MPP) has today announced a new, royalty-free licence agreement with AbbVie for glecaprevir/pibrentasvir (G/P) - a World Health Organization (WHO)-recommended treatment for people living with chronic hepatitis C (HCV). The licence will enable quality-assured manufacturers to develop and sell generic medicines containing G/P in 99 low- and middle-income countries (LMICs) and territories at affordable prices, enabling access to and treatment scale-up with the most effective pan-genotypic regimens. The agreement was launched at the American Association for the Study of Liver Diseases (AASLD) The Liver Meeting 2018 in San Francisco.
"G/P is a priority therapy for licensing for the MPP, so this agreement with AbbVie is very good news for public health," said Dr Marie-Paule Kieny, Chair of the MPP Governance Board. "It is a really important new option for a significant proportion of HCV patients throughout the world. As with previous MPP licences, we look forward to facilitating access to generic versions of this product as quickly as possible in as many territories as possible."
Globally, 71 million people are currently living with chronic HCV, many of them in LMICs. By the end of 2015, only 20 percent had been diagnosed and a mere seven percent of them had received treatment. In February 2017, the MPP issued its annual report on priority medicines for in-licensing. Given its favourable clinical profile and high potential in LMICs, G/P was listed as a key priority treatment.
G/P is an all-oral, once-daily, pan-genotypic combination regimen and was originally approved in 2017. It has achieved high cure (SVR12) rates of 98 per cent in treatment-naïve non-cirrhotic patients across all six genotypes of the virus. It is recommended by the WHO as a first-line treatment for eight weeks in treatment- naïve non-cirrhotic patients. Treatment-naïve patients with compensated liver cirrhosis require a 12-week treatment course.
Further, the regimen is also indicated for use in HCV patients with any degree of renal impairment, including patients on dialysis. Globally between five and ten percent of all people living with chronic HCV infection are estimated to be living with kidney disease and this treatment will be very helpful for them.
There are 95 countries and four territories included in the MPP/AbbVie licence for G/P at this point.
More details: www.medicinespatentpool.org
What the MPP's partners are saying:
"Central to our vision at AbbVie is developing therapies, such as our pan-genotypic HCV treatment, for the most serious diseases and providing access to those treatments. We are pleased to have reached today's agreement with the MPP."
Laura Schumacher, Executive Vice President, External Affairs, General Counsel and Corporate Secretary, AbbVie
"The new agreement is an important step towards achieving elimination of hepatitis C worldwide. We urge national governments to take action now to make such curative treatments available for the millions of people in need."
Dr Gottfried Hirnschall, Director of Department of HIV and Global Hepatitis Programme, World Health Organization
"Unitaid aims to maximise the public health response by enabling equitable access to better health for all. We welcome this agreement between the MPP - a Unitaid grantee - and AbbVie that will accelerate a more effective HCV response worldwide."
Lelio Marmora, Executive Director, Unitaid
"Claiming over one million lives each year, viral hepatitis is one of the world's major public health challenges and disproportionately affects people living in LMICs. Therefore access to safe, quality-assured treatments, affordable for all, has to be the fundamental aim of the public health community. This is a big step in that direction. The next step is to see more territories included in the agreement. Each step makes the dream of hepatitis C elimination more real."
Raquel Peck, CEO, World Hepatitis Alliance
"The Government of Pakistan warmly welcomes the agreement between the Medicines Patent Pool and AbbVie to expand access to glecaprevir/pibrentasvir - a very important therapy for the treatment of HCV - into territories including Pakistan. The HCV burden in Pakistan is endemic, affecting over eight million of our country's population and the prevention and treatment of HCV is a national priority. This agreement will considerably aid our efforts and, ultimately, accelerate the permanent elimination of the HCV virus."
Mr Aamer Mehmood Kianai, Ministry of National Health Services, Regulations and Coordination, Government of Pakistan
The MPP has an existing collaboration with AbbVie and has two agreements in place in the field of HIV. These are:
- Licence on paediatric formulations of lopinavir/ritonavir, signed in November 2014, which is facilitating the development of improved paediatric formulations for at least 102 LMICs
- Licence on adult formulations of lopinavir/ritonavir for use in Africa, signed in December 2015.
In HCV, the MPP has agreements with Bristol-Myers Squibb on daclatasvir and Pharco on ravidasvir.
About the Medicines Patent Pool
The Medicines Patent Pool is a United Nations-backed public health organisation working to increase access to, and facilitate the development of, life-saving medicines for low- and middle-income countries. Through its innovative business model, the MPP partners with civil society, governments, international organisations, industry, patient groups and other stakeholders, to prioritise and license needed medicines and pool intellectual property to encourage genetic manufacture and the development of new formulations. To date, the MPP has signed agreements with nine patent holders for thirteen HIV antiretrovirals, one HIV technology platform, three hepatitis C direct-acting antivirals and a tuberculosis treatment. The MPP was founded and is funded by Unitaid.
Abbvie's MAVIRET (glecaprevir/pibrentasvir)
EU Indication
MAVIRET is indicated for the treatment of chronic hepatitis C virus (HCV) infection in adults.
Important EU Safety Information
Contraindications:
MAVIRET is contraindicated in patients with severe hepatic impairment (Child-Pugh C). Concomitant use with atazanavir containing products, atorvastatin, simvastatin, dabigatran etexilate, ethinyl oestradiol-containing products, strong P-gp and CYP3A inducers, such as rifampicin, carbamazepine, St. John's wort, phenobarbital, phenytoin, and primidone.
Special warnings and precautions for use:
Hepatitis B virus reactivation
Cases of hepatitis B virus (HBV) reactivation, some of them fatal, have been reported during or after treatment with direct-acting antiviral agents. HBV screening should be performed in all patients before initiation of treatment.
Hepatic impairment
MAVIRET is not recommended in patients with moderate hepatic impairment (Child-Pugh B).
Patients who failed a prior regimen containing an NS5A- and/or an NS3/4A-inhibitor
MAVIRET is not recommended for the re-treatment of patients with prior exposure to NS3A/4A and/or NS5A-inhibitors.
Adverse Reactions
Most common (≥10%) adverse reactions for MAVIRET were headache and fatigue.
Globally, prescribing information varies; refer to the individual country product label for complete information.
SOURCE Medicines Patent Pool via www.natap.org
Liver Cancer (HCC) Treatment Options

One of the feared complications of Hepatitis C is HepatoCellular Carcinoma (HCC) aka Liver Cancer. While anyone can get this type of cancer it is most common in patients who have liver cirrhosis from any cause. We look for it using a blood test for AlphaFeto Protein (AFP) and/or Ultrasound, CT or MRI.
Ok, so the news has come back that you have an HCC. What are the treatment options?
- Do Nothing
- Chemotherapy with Sorafenib or Cabozantinib
- RFA
- TACE
- Resection
- Transplantation
- Experimental/Unproven/Deprecated Procedures
For a detailed rundown of current best practice please see https://bestpractice.bmj.com/topics/en-us/369
For a brief executive summary, please read on.
Do Nothing
While this sounds (and is) very nihilist the reality for some unfortunate patients is that nothing we do is likely to help.
Chemotherapy
Sorafenib, and more recently Cabozantinib are tyrosine kinase inhibitors. They are both tablets and can both slow down the progression of HCC in some patients. The key words are "slow down" and "in some patient" because neither drug can cure the HCC and they don't work in all patients.
Details on Sorafanib can be found here: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2702892/
Details on Cabozantinib (the new kid on the block) can be found here: https://www.nejm.org/doi/full/10.1056/NEJMoa1717002
While Cabozantinib is probably better than Sorafanib, it is yet to be widely available. I have had a single patient who was already failing Sorafenib get 2 good extra years on Cabozantinib, but eventually, that too failed.
RFA
RFA stands for Radio Frequency Ablation. The simplest way to look at it as like this. We have a needle we stick into the tumour and the tip of it is like a miniature microwave oven. We then switch this on an cook the surrounding tissue. The idea is to kill all the cancer tissue and the minimal amount of surrounding healthy tissue. All things going well it can cure an HCC. For more details on the procedure: https://en.wikipedia.org/wiki/Radiofrequency_ablation
And for an analysis of the success rates: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5011083/
TACE
TACE stands for Trans Arterial Chemo Embolisation. It is a little like RFA but in this case the "needle" is flexible, and rather than stick it straight through the skin we thread it up through an artery. This bit is similar to an angioplasty for the heart. We continue threading it up the arteries until we find the artery that is supplying the tumour. We then inject some stuff to block off this artery and release some very toxic routine chemotherapy medications (doxorubicin or cisplatin). The idea is that everything downstream is killed. All things going well it can cure HCC. For more details on the procedure: https://en.wikipedia.org/wiki/Transcatheter_arterial_chemoembolization
And for an analysis of the success rates: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4915316/
Resection
If the HCC is in a favourable position in the liver it may be possible to cut it out. You don't need all your liver so throwing a segment, or a 1/2 of it out is possible.
Transplantation
Where resection is not possible, complete replacement of the liver may be possible. This becomes impossible if the tumour invades vital structures like the blood supply pipes or the bile ducts. Transplantation is complicated, expensive, requires long term immune supression, and there are not enough donor livers or transplant centers available.
Experimental/Unproven/Deprecated Procedures
TARE
TARE stands for Trans Arterial Radio Embolisation and in principle is like TACE except instead of chemotherapy laden spheres being use, radioactive spheres are used. For more information https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5497664/
Ethanol Ablation
The technique of Ethanol Ablation is similar to that of RFA in that a needle is inserted into the tumour through the skin, thus the other name PAE (Percutaneous Alcohol Ablation). It has largely fallen out of favour as it is not as effective as RFA and has more side effects. For more information https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3296972/
Naturopathy
It remains possible that there are natural medicines, largely unknown to science that may impact on HCC. I am personally aware of one patient who appears to have been cured using this modality.
Recurrence
The sad reality is that the cirrhosis that predisposes to getting one HCC predisposes to getting another, so curing one fixes the immediate problem, but more tumours may appear in the future. Long term follow up and monitoring is vital.
Hepatitis C and HCC
In the context of having Hepatitis C it's important to treat the HCC first, then treat the Hep C. For more details please see https://fixhepc.com/blog/item/108-daas-and-hcc-when-to-do-what-in-plain-english.html
The Good News Front
Without SVR one study showed liver cancer rates of 2.63% per year falling to 0.55% per year so Hep C treatment drops the risk of HCC development to about 1/5 of what it is untreated.
Hep C Guidelines - An Executive Summary
Detailed expert guidelines are great but often run to hundreds of pages meaning it can be hard to find the specific information you want.
Giten Khwairakpam from TREAT Asia / amfAR just shared this awesome executive summary with me, so I'm sharing it here with you.
As a part of TREAT Asia/ amfAR’s efforts to increase access to hepatitis C and HIV co-infection diagnosis and treatment, we are pleased to share a new fact sheet that summarizes and simplifies key updates from the July 2018 version of the WHO Guidelines for the Screening, Care, and Treatment of Persons with Hepatitis C Infection. It can be accessed at https://www.amfar.org/guidelines/.
A full list of our hepatitis-related resource materials is available at https://www.amfar.org/facts/
We hope that this fact sheet will be useful for treatment advocates, primary care physicians and public health experts in understanding the recommendations better and help in shaping implementation strategies.